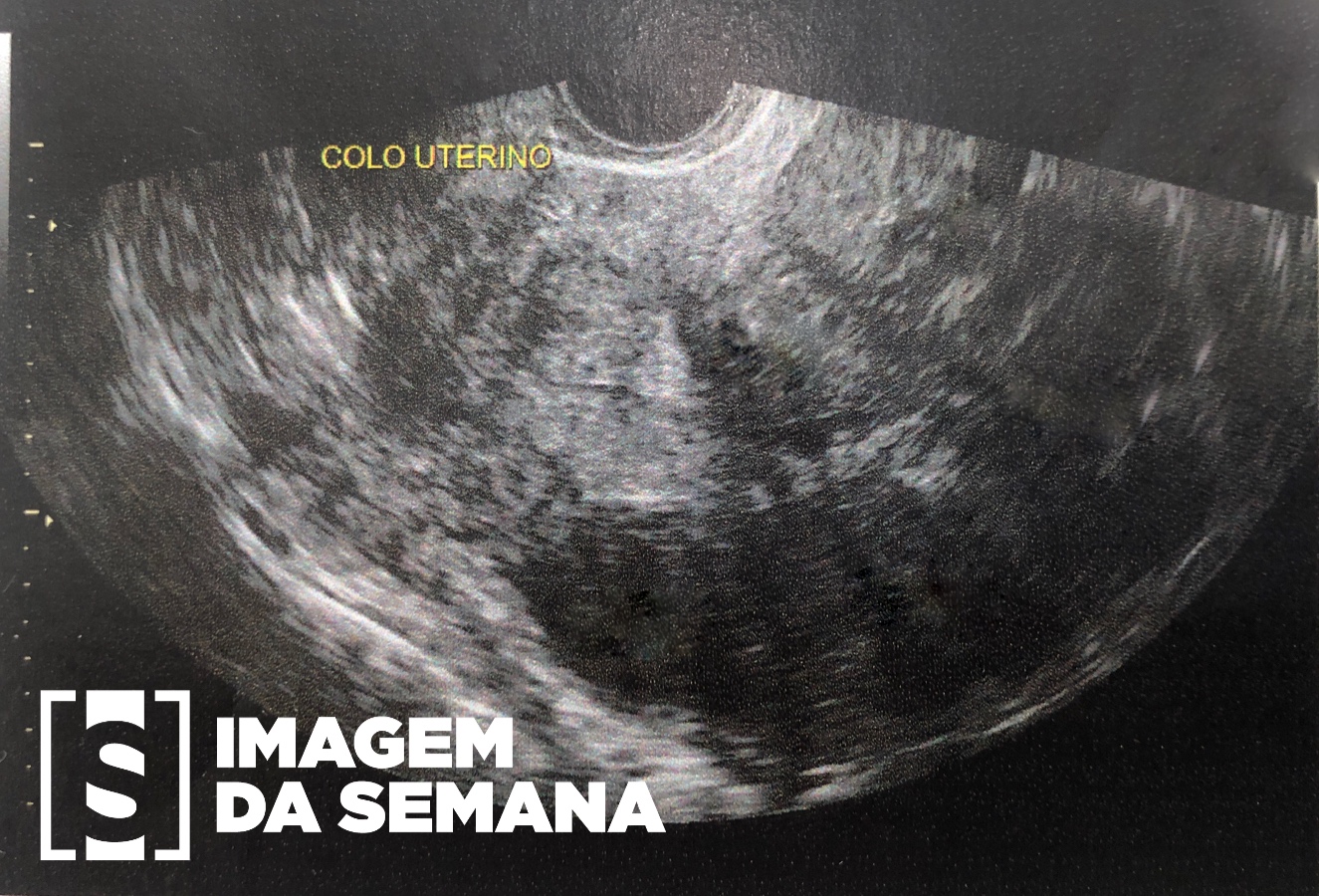
Case 425 Medical history Image 1: transvaginal ultrasound, without doppler, uterine level. Case description A 42-year-old female patient, G7P1A6, presenting dysmenorrhea (10/10 intensity), menorrhagia, polymenorrhea, and pollakiuria for over the past 5 years, has been feeling indisposed recently. Denies dyspareunia. She also reports having one alive child and 6 abortions, with two being in vitro fertilizations, both unsuccessful. Despite that, it is not her desire to get pregnant again. Negative familiar history of uterine cancer. On physical exam: bleached patient, palpable pelvic masses present. Transvaginal ultrasound was requested (TVS). Question Based on the patient’s clinical condition and the image exam, which is the most likely diagnosis and the main course of action to take? Uterine leiomyosarcoma, uterine artery embolization Endometrial adenocarcinoma, hysterectomy Uterine leiomyomatosis, hysterectomy Endometrial polyps, expectant conduct Test question (UNIFESP - SP - 2010 - R1 - 1) A patient presents to the hospital with hematocrit of 24%. The transvaginal ultrasound indicates the presence of a 14 cm pedunculated myoma in the uterine fundus, with numerous smaller submucous myomas. The initial approach should be: hysteroscopic myectomy uterine artery embolization blood transfusion total hysterectomy and bilateral salpingo-oophorectomy GnRH agonist for 3 months, combined with ferrous sulfate Time is Up! Time's up