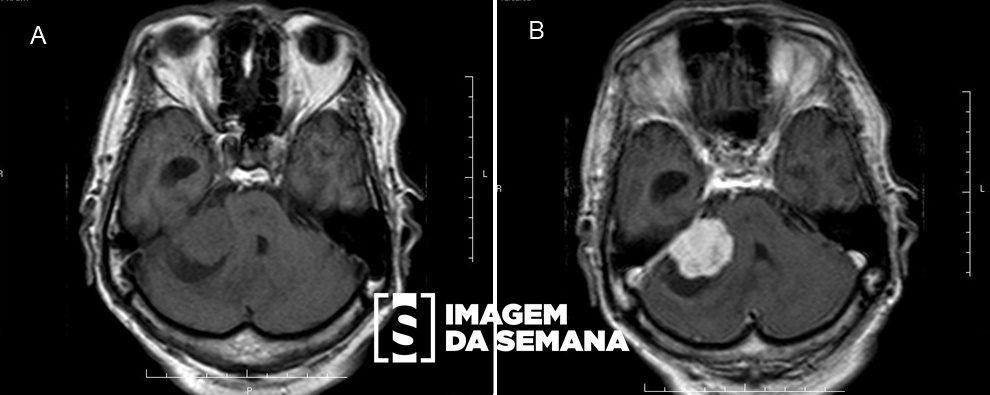
Case 391 Medical history Male patient, 21-years-old, reports fatigue, dizziness and dyspnea during usual activities. No comorbidities reported. Physical examination showed lower limb edema, a visible apex beat palpable with 3 digitals, grade II Levine proto systolic murmur, an elevate jugular venous pressure, tender hepatomegaly, and lesions as observed in Image 1. Further propaedeutic revealed ejection fraction of 35% and the radiologic findings as seen in Images 2 and 3. The diagnosis was tuberous sclerosis complex (TSC). Photograph of the patient’s face.Brain Computed Tomography (CT), without intravenous contrast, showing axial planes at the level of lateral ventricles bodies (a) and high frontoparietal convexity (b).Brain CT, without intravenous contrast, showing coronal reconstruction, at the level of 3rd ventricle.Chest radiograph in posteroanterior incidence (a) and in lateral view (b), both in orthostatism.Question:Considering the clinical history and images presented, which typical finding of this diagnosis was NOT seen in this case? Cortical tubers Cardiac rhabdomyomas Angiofibromas Supependymal nodules Test question (SBP, 2008 - adapted) A nine-months-old patient, that presents epileptic seizures since the second month, is hospitalized with signs and symptoms of heart failure. Physical examination shows hypopigmented macules, leaf-like shaped, distributed in trunk and proximal parts of superior limbs. Echocardiogram shows the presence of an intracavitary nodule attached to the anterior wall of the left atrium.Question:The most likely diagnosis is: Neurofibromatosis Tuberous sclerosis complex Endocardial fibroelastosis Velocardiofacial syndrome Time is Up! Time's up