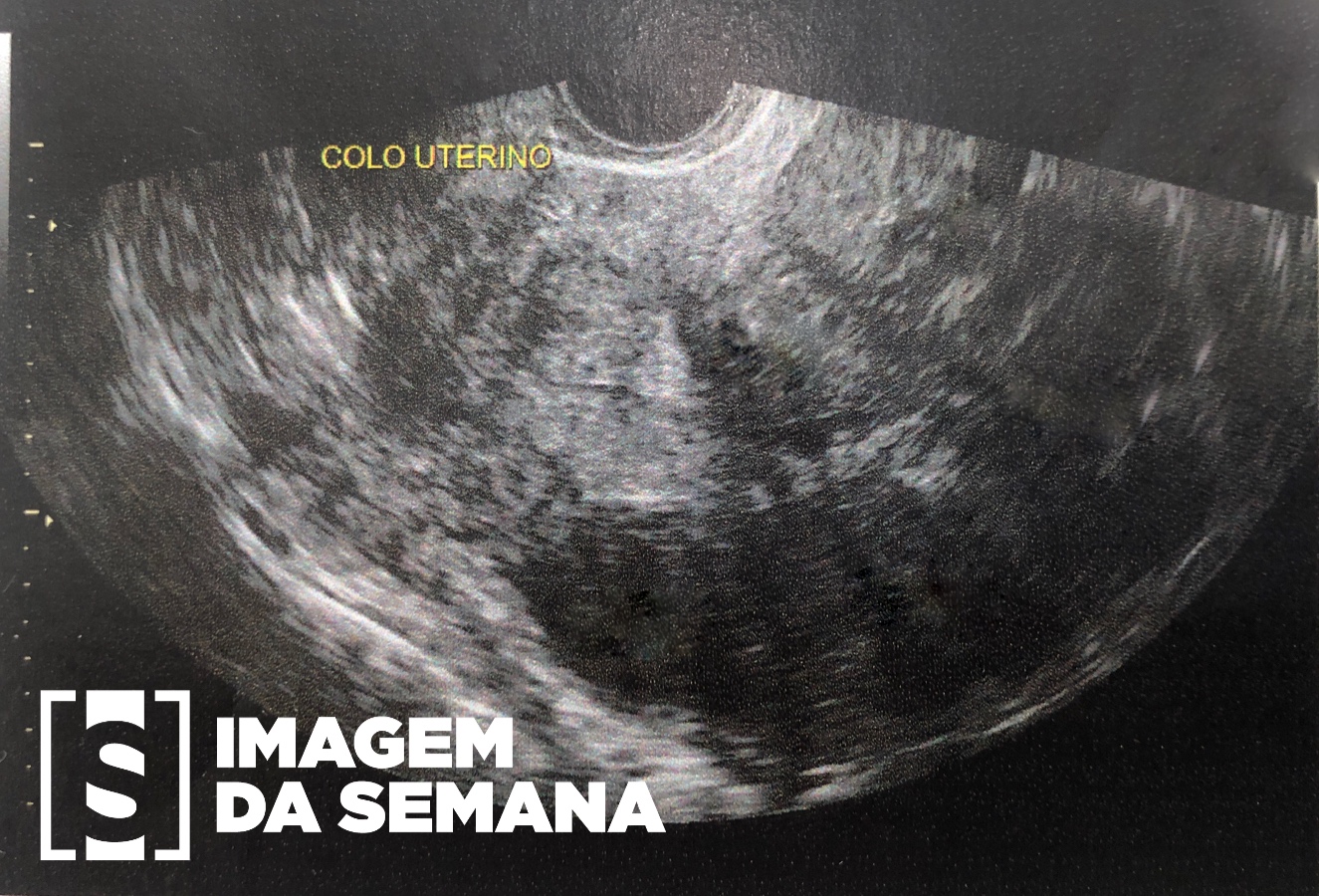
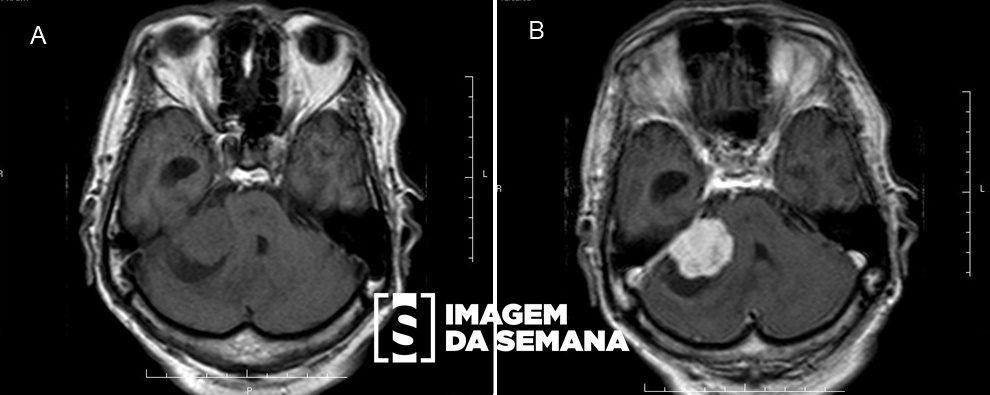
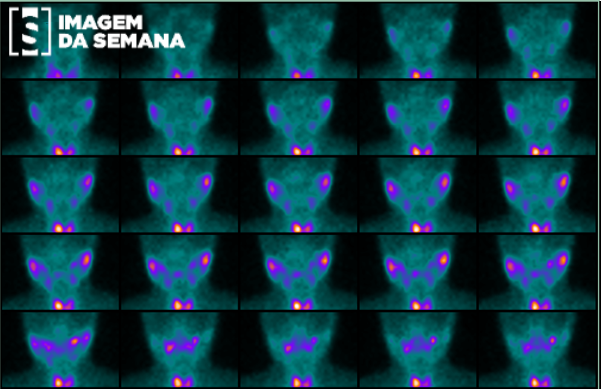
Case 376 Medical History A 57-year-old female patient initiated diffuse bone pain over a year ago and was admitted to the hospital after presenting with worsening of symptoms, which restricted deambulation. Laboratorial findings showed calcitonin: 15,4mg/dL (reference range: 8,5-10,2mg/dL), PTH: 2566,8pg/mL (reference range: 18,5-88,0pg/mL) and alkaline phosphatase: 1525U/L (reference range: 36-110 U/L). Computed tomography (CT) and magnetic resonance imaging (MRI) of the neck were performed. After hemodynamic and calcium levels stabilization, the patient underwent surgical resection of the lesion. Computed tomography (CT) - (A) and magnetic resonance imaging (MRI) of the neck, weighed in T2, sagittal section, at the median line (B).Computed tomography (CT) of the neck, axial section, at the superior thoracic aperture, before (A) and after (B) intravenous contrast injection.Axial computed tomography (CT) imaging of the neck, reconstructed in soft tissue window, before (A) and after intravenous contrast injection (B), and reconstructed in bone window (C). Axial MRI imaging of the neck, weighed in T2 (D) and in T1 (E). The images were acquired at the mandible level.Surgical sampling photography (A) and microscopy images of hematoxylin-eosin stained slides (B) Question:Considering the clinical history and images presented, what is the most likely diagnosis? Thyroid carcinoma Parathyroid carcinoma Parathyroid adenoma Thymoma Test Question COMISSÃO ESTADUAL DE RESIDÊNCIA MÉDICA DO AMAZONAS – AM 2016 In primary hyperparathyroidism, we may find: Augmented levels of calcium and PTH. Augmented levels of PTH and diminished levels of serum calcium. Diminished levels of PTH and calcium. Diminished levels of PTH and augmented levels of serum calcium. Previous Next Next Time is Up! Time's up