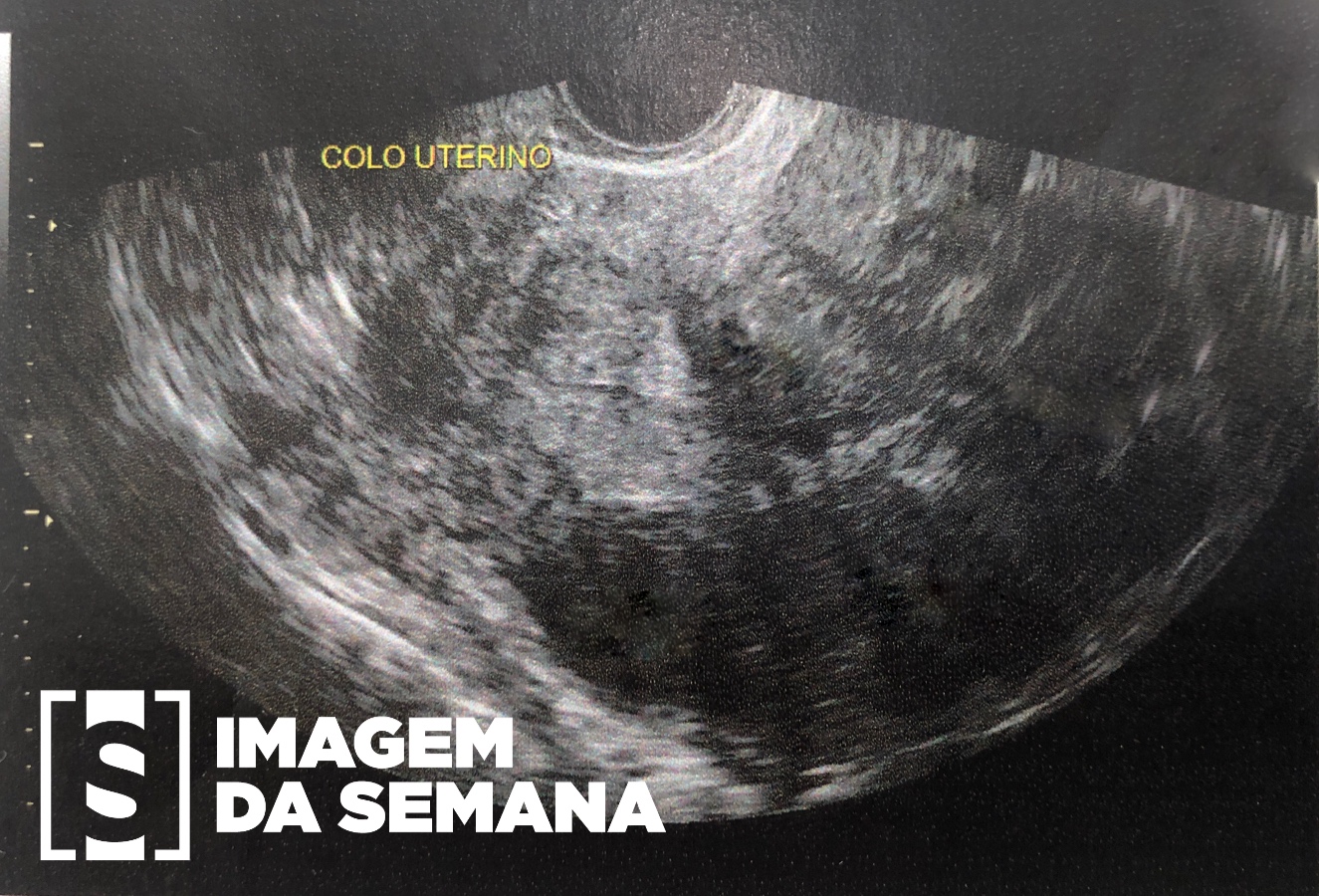
Case 328 Medical history Female patient, 39 years old, asymptomatic, with 33 weeks of her first pregnancy. Denies comorbidities. Low-risk pregnancy, with normal previous gestational ultrasound (US). Current ultrasound examination reveals: female fetus and abdominal cystic formation (Images 1 and 2). Image 1: Obstetric ultrasound (US) of the third trimester.Image 2: Obstetric ultrasound (US) of the third trimes Question:Considering the clinical history and the images presented, what would be the most appropriate conduct for the case reported? Puncture of the cyst. Request magnetic resonance imaging (MRI) for better characterization of the lesion. Expectant conduct, with serial ultrasounds. Anticipation of childbirth. Test Question (Medical Residency - UFPR) A 26-year-old female patient, nulliparous, comes for gynecological consult, reporting low-intensity pelvic pain in the left iliac fossa. Sexarch at age 21, has regular menstrual cycles, does not use oral hormonal contraceptive. Contraceptive method used: condom. Little sexual activity and negative surgical history. Specular examination without alterations. Vaginal touch: Cartilaginous cervix, anteversion of the uterus, normal size. Sensation of mobile mass in the left attachment. You request endovaginal pelvic ultrasound: uterus in anteversion. Volume of 70 cm³. Endometrium 6 mm. Right ovary with 6 cm³ volume. Cyst in the left ovary, smooth walls and without septations, measuring 8 cm. Question:From this picture, what is the proper conduct? Expectant conduct; repeat the endovaginal ultrasound at 8 weeks. Indicate laparotomy and do left anexectomy. Indicate videolaparoscopy and perform ovarian cystectomy. Prescribing gosserelin acetate 10.8 mg subcutaneously every 3 months. Prescribe anastrozole 1 mg / day, orally for 6 months and repeat endovaginal ultrasound. Previous Next Next Time is Up! Time's up