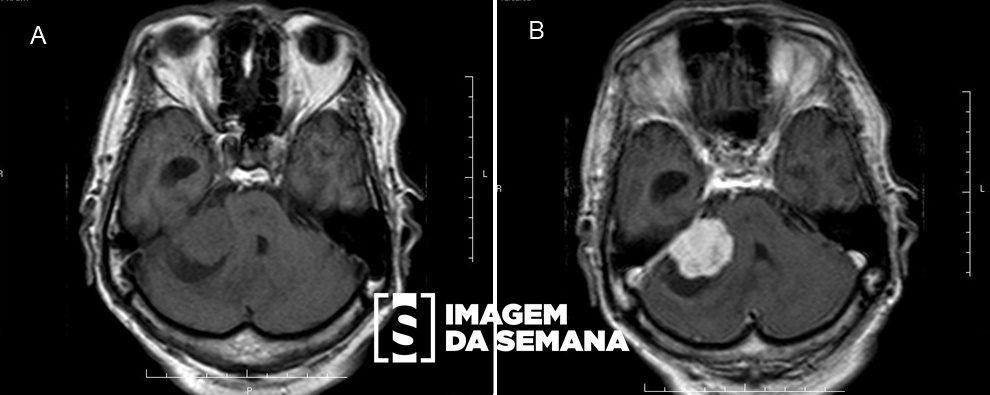
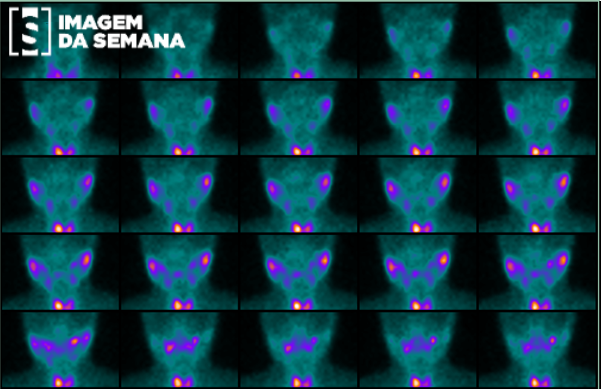
Case 282 Medical History A 52-year-old male patient sought medical attention with severe throbbing headache and vomiting, with progressive worsening during the last week. He is in treatment for hypertension with losartan 50 mg daily and has a history of unilateral left hearing loss for 8 months. Physical examination: ataxic gait, falls arising from orthostatic position, symmetrical face, hypoesthesia in the left hemiface. Magnetic resonance imaging (MRI) of the brain was requested. Image 1: Magnetic resonance imaging (MRI), weighted in T1, left paramedian sagittal cut, without intravenous contrast medium (gadolinium).Image 2: Magnetic resonance imaging (MRI), weighted in T1, axial cut, internal auditory meatus level, after intravenous injection of gadolinium.Image 3: Magnetic resonance imaging (MRI), sequential axial weights, T2-weighted, no intravenous contrast medium (gadolinium), internal auditory meatus and membranous labyrinths levels.Image 4: Magnetic resonance imaging (MRI), sequential coronal sections, T2-weighted, without intravenous contrast medium (gadolinium), internal auditory meatus level. Question:Analyzing the clinical case and the images presented, what is the probable diagnosis? Schwannoma Meningioma Epidermoid cyst Jugulotimpanic paraganglioma Test Question [SEAP/SES-NS, 2014]Considering the imaging investigation of sensorineural hearing loss, mark the correct alternative. The negative result of computed tomography (CT) excludes the presence of retrocochlear lesions due to the high sensitivity it presents. For the investigation of the VIII cranial nerve Schwannoma, the image examination indicated is the simple radiography. In the suspected Schwannoma of the VIII cranial nerve, confirmation with magnetic resonance imaging is necessary, especially when the lesion is restricted to the internal auditory canal. High resolution computed tomography (HRCT) has low specificity for the identification of foci of otosclerosis in patients with clinical suspicion. The presence of the vestibulocochlear nerve in the internal auditory canal can only be confirmed by means of helical CT. Time is Up! Time's up