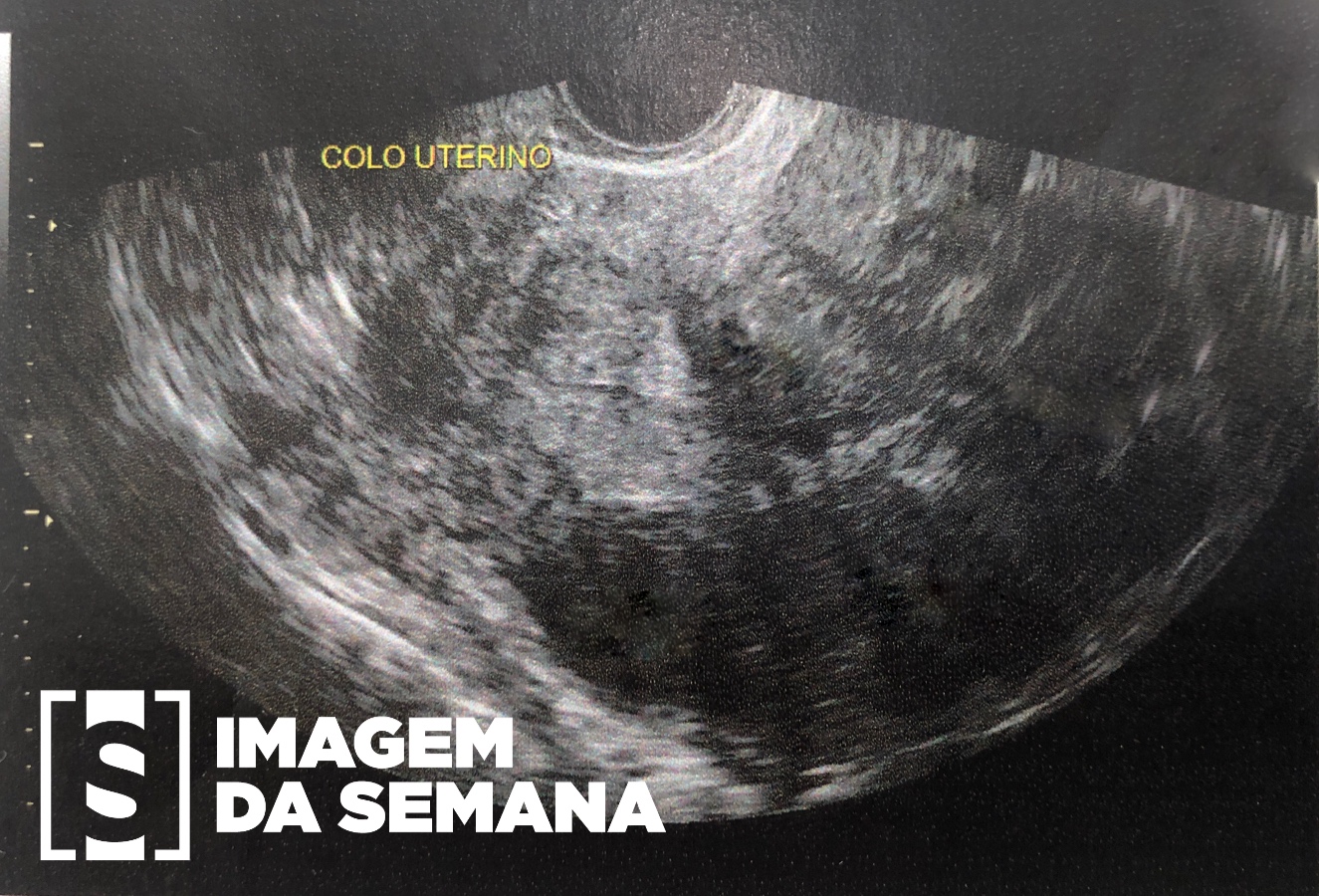
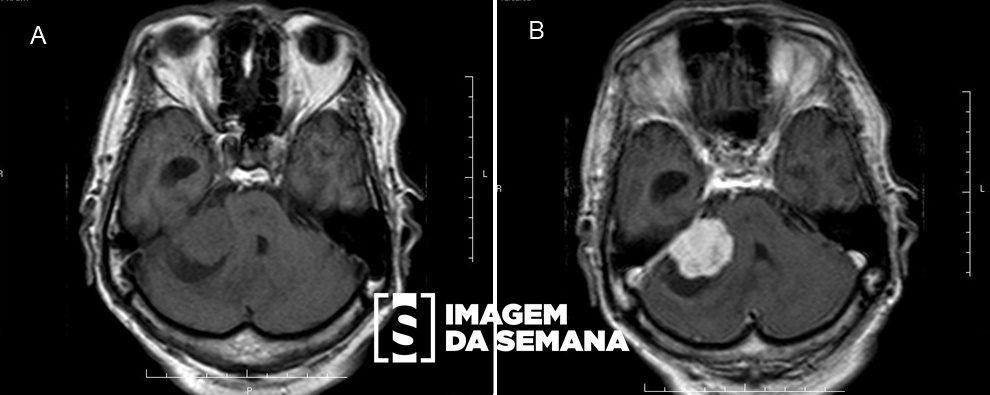
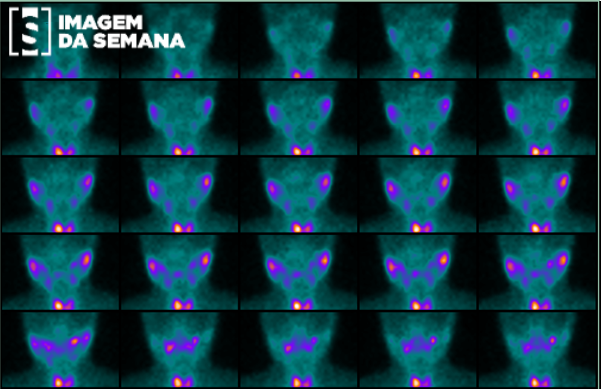
Case 125 Medical History A two-month-old female child was admitted at an emergency department for persistent jaundice, acholic stools and choluria. Laboratorial data included: hemoglobin: 8.11; hematocrit: 22.8, gammaglutamyl transferase: 1262; alkaline phosphatase: 612; aspartate aminotransferase: 105; alanine aminotransferase: 33; total bilirubin: 5.4; direct bilirubin 3.8. On physical examination, she presented mucosal pallor, enlarged abdomen, a liver edge palpable 6 cm below the right costal margin and mild splenomegaly. An abdominal ultrasonography (US) was then requested. Image 1: Doppler scan of the portal bifurcation. Image 2: A right upper quadrant US view showing the gallbladder. Image 3: A left upper quadrant US view showing the spleen. Question:Which is the standard management for this condition? The absence of a band-like periportal echogenicity in the ultrasonographic imaging (triangular cord sign) is enough to rule out the diagnosis of biliary atresia and investigation should now focus on clinical conditions. Phototherapy and clinical assessment with daily serum bilirubin testing should be provided. Hyperbilirubinemia is a normal finding at this age and serum bilirubin levels might be markedly high until the child is 6 months old. The patient should undergo exploratory laparotomy in order to confirm the diagnosis of biliary atresia. If such diagnosis is made, the child should also be surgically treated using the Kasai procedure. Previous Next Next Time is Up! Time's up