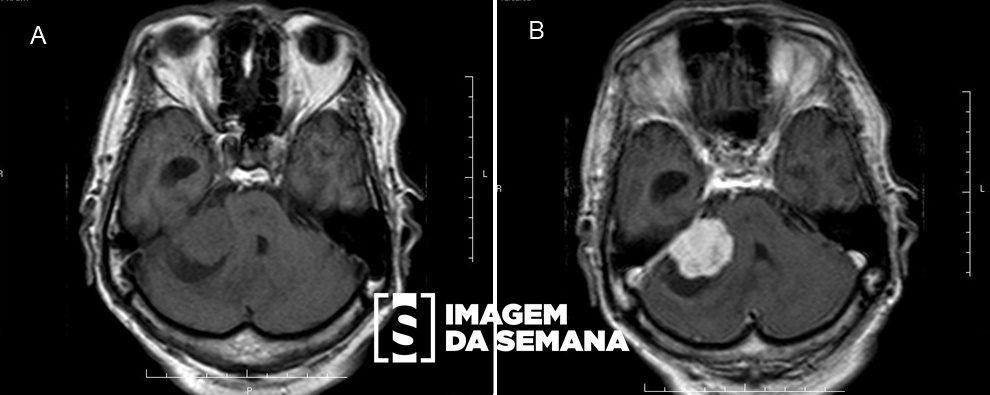
Case Medical history A 65-year-old male patient, hospitalized after sudden episode of vertigo, nausea and dysarthria, with rapid evolution to hemiplegia and a decreased level of consciousness in 24 hours. At physical examination, the patient was afebrile with complete bilateral horizontal gaze palsy and dysdiadochokinesia. His medical history shows a longtime smoker and a poorly controlled high blood pressure. To the initial evaluation was request cranial computerized tomography (CT) scan, lumbar puncture and electroencephalogram (EEG). Image 1: Cranial CT scan, without contrast, axial image at level of the ponsImagem 2: Electroencephalogram (EEG) report:  The awake electroencephalogram was obtained in satisfactory technical conditions with 30 minutes of record. The background activity is well-organized and symmetrical. Posterior dominant rhythm was observed with 10 to 12 Hz of frequency and 20 to 80 µV of amplitude, with appropriate reactivity to the opening and closing of the eyes. In the other regions, the background activity consists of theta and beta waves.Imagem 3: Cerebrospinal fluid (CSF) analysis:  Color and turbidity: Clear and colorless N° of cells: 2/mm³ White-cells profile: Lymphocytes-63%;Monocytes-37% Proteins: 32 mg/dL Glucose: 60 mg/dL(67% of capillary glycemia) Lactate: 13 mg/dL Question:Based on clinical history and on examination of the test results, the most likely diagnosis is: Exogenous poisoning Meningoencephalitis Status epilepticus Basilar artery thrombosis None Time's up