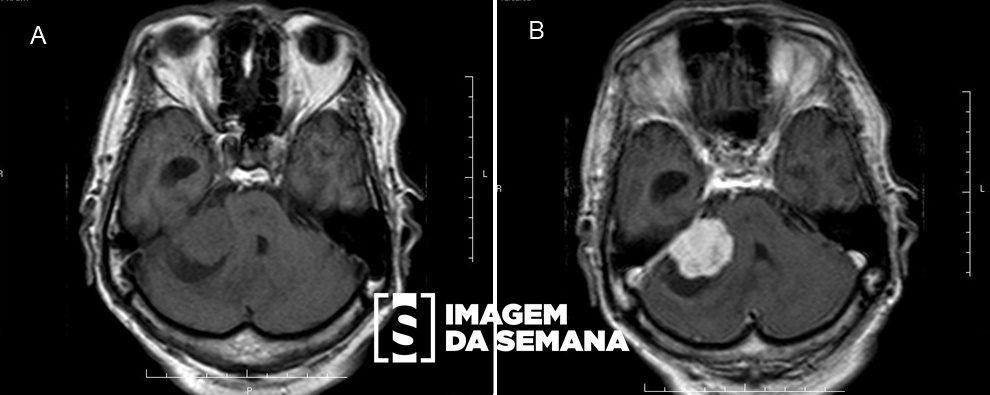
Case 288 Medical History A 65-year-old female patient was referred by the Emergency Care Unit due to sudden headache in fron-tal and occipital areas initiated in the last 24 hours, associated with vomiting and loss of consciousness. Presented hypertensive spikes during hospitalization as well as photophobia, nuchal rigidity and pain on cervical mobilization. She is a former smoker (60 pack-years, interrupted use for 9 years), with a social drinking habit and hypertension (losartan suspended for 3 years by medical guidance). Computed tomo-graphy (CT) of the brain was performed during the first care - attached. Computed tomography (CT) of the brain, without intravenous injection of contrast medium. Computed tomography (CT) of the brain, without intravenous injection of contrast medium. Question:Given the clinical case and the images provided, what is the diagnosis and the preferred exam for the im-mediate decision in the clinical conduction of this patient? Chronic subdural hematoma - Computed tomography (CT). Hypertensive intracerebral haemorrhages - Magnetic resonance imaging (MRI). Acute subarachnoid hemorrhage - Cerebral CT angiography. Reversible cerebral vasoconstriction syndrome - Conventional angiograpy. None Test Question (HSJJ - São José de Joinville Hospital / 2011) MRC, a female student, is attended at the emergency room of the hospital with a report of sudden severe headache, followed by ptosis, mydriasis, non-photorreative and divergent strabismus on the right. The cranial CT scan revealed subarachnoid hemorrhage in cisterns at the base of the skull.Question:The most likely diagnosis and the conduct to be taken by the attending physician should be: Cerebral infarction: watchful waiting. Cerebral contusion: indication of craniotomy. Cerebral aneurysm: arteriography of cerebral vessels. Intracerebral hematoma: indication of craniotomy. Subdural hematoma: drainage using a trephine craniotomy. None Time's up